The traditional method of choice would be, a BSSO and setback of the mandible with rotation on the z axis, followed with a 3-piece LeForte I on the maxilla with differentiated intrusion to correct the cant of the upper jaw.
However the authors suggest a less invasive approach with an intraoral vertical ramus osteotomy and setback-rotation on the mandible, and an approach with miniscrews and intrusion on the maxilla to correct the canting on the upper.
Let's take a minute and describe a vertical mandibular osteotomy and then see the results of the case shown on the above article.

In this sketch the Vertical Mandibular Osteotomy is shown, to set back the mandible, the posterior part is pushed laterally, and the anterior part is the pushed in and posteriorly.
Case Report:
Patient with Class I skeletal relationship, with a canted upper posterior occlusal plane, and a mandible deviating to the left. Patient is found with TMD symptoms on his left joint.

Canted occlusal plane and mandibular deviation clearly visible, on his initial frontal X-Ray.

This is the system applied in the presurgical orthodontics to create a leveled occlusal plane posteriorly on the maxillary dentition. A titanium miniscrew is inserted on the zygoma, with a metal ligature and a power chain to th 7+4 segment to intrude. For anchorage purposes and to not allow any buccal flaring of the segment a TPA is applied.

On the pre-surgical frontal, you can evaluate the correction of the cant (blue line) when compared with the initial canting (white line). The above described vertical ramus osteotomy, with mandibular set-back and rotation is performed.

Final result after surgery with correction of the mandibular deviation.
Concerning the TMD on the left joints symptoms were eliminated after surgery, and an idea of the result could be seen on the tracing of the mandibular movements on the condyle level before and after surgery (bare in mind the mandibular lateral displacement is one of the few evidence based proved, occlusal pre-disposal factors for TMD)

Before treatment, you can evaluate the difference of the movement when patient is chewing left and right. (first tracing is the midline, second is the right condyle and third row is the left condyle)
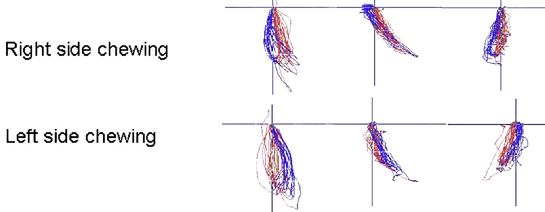
The result post treatment, pre-surgical orthodontics and surgery. (first tracing is the midline, second is the right condyle and third row is the left condyle)
Conclusion:
keeping in mind that this is not a high level of evidence, but a single case report, this approach shows promising results on this certain case. Further analysis of similar cases and the treatment outcome of those could give further evidence.
Also when compared with a traditional double jaw, with 3-piece maxilla, procedure approach, the above is certainly less invasive, and should be also pointed out.
D.G.
Reference Articles:

Great Blog. The method explained is quite different from the traditional one. The results are also better.
ReplyDeleteMichigan cosmetic dentist
There is similar approaches in younger individuals, with Hyrax instead of a TPA, and miniscrews to intrude the segments. Although Hyrax is a more rigid appliance, tipping of the buccal segments is seen often. The loosening of the suture could be one explanation.
ReplyDeleteWhat makes this approach interesting is the surgical procedure of setting back the mandible, without a conventional BSSO.
Thank you for your comment
This technique requires more time to show its results and effectiveness.
ReplyDeleteJason West
I'm not sure I understood your comment Jason.
ReplyDeleteIf you mean that intrusion takes time, I must say that with light forces and a segmented approach intrusion does not take so much time. Also increasing occlusal forces helps towards that goal.
Perfect hygiene and light forces. For example for intrusion of 4 incisors on the upper you do not need more than 25-50gr of force, with a three piece Burstone approach. Try with a dynamometer and check how light such a force is.
I examine your blog site presently share great information right below. Advanced Dental Treatment
ReplyDeleteThanks for the blog.Nice mandibular deviation and canted information.You can also check.
ReplyDeletemandibular deviation and canted